Dislocated Elbow by Trenee Calamia
Mechanism Of Injury
- Occurs most often by either a fall on the outstretched hand with the elbow in or
poistion of hyperextension, (which happened to me) - Or by a sever twist while the elbow is in a flexed position. (Most common is
posterioly)
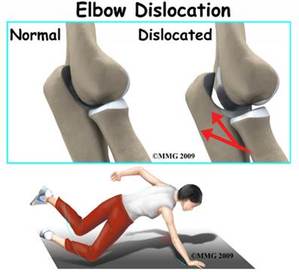
Structures involved
The bones of the ulna & radius may be displaced backward, forward, or
laterally.
Signs and Symptoms
Treatment (Tx)
Corrective Technique
After reduction, the physician will often immobilize the elbow in a position of flexion & apply a sling suspension
Rehabilitation
Injury can lead to…
Prolonged derangement of soft tissue if not tended to immediately.
laterally.
- Most common is when both the ulna & radius are forced backward.
- The Olecranon Process extends posteriorly well beyond its normal alignment with the humerous.
- The forward displacement of the ulna & radius appear deformed.
Signs and Symptoms
- Elbow dislocations involve rupturing and tearing most of the stabilizing ligamentous tissue, accompanied by profuse hemorhage and swelling.
- There is severe pain and disability.
- The complications of such traumas include injury to the median & radial nerves as well as to the major blood vessels & arteries and in almost every instance include myositis ossification.
- Elbow dislocation is often associated with a radial head fracture.
Treatment (Tx)
- The primary responsibility is to apply cold & pressure immediately. Then a sling, & to refer the patient to a physician for reduction.
- The neurovascular status of a brachial artery & the median and ulnar nerves must be evaluated before and after reduction.
- Only a physician should reduce an elbow dislocation.
- It must be performed as soon as possible to prevent prolonged derangement of soft tissue.
- In most cases, the physician will administer an anesthetic before reduction to relax muscle spasms.
Corrective Technique
After reduction, the physician will often immobilize the elbow in a position of flexion & apply a sling suspension
Rehabilitation
- Keep in sling for approx. 3 weeks.
- The length of immobilization should be minimized if the ulnar collateral ligament is intact & stable.
- While the arm is maintained in flexion, the patient should execute hand gripping & shoulder exercises.
- Once initial healing has occurred, heat & gentle, passive exercise may be applied to help gain full ROM.
Injury can lead to…
Prolonged derangement of soft tissue if not tended to immediately.
